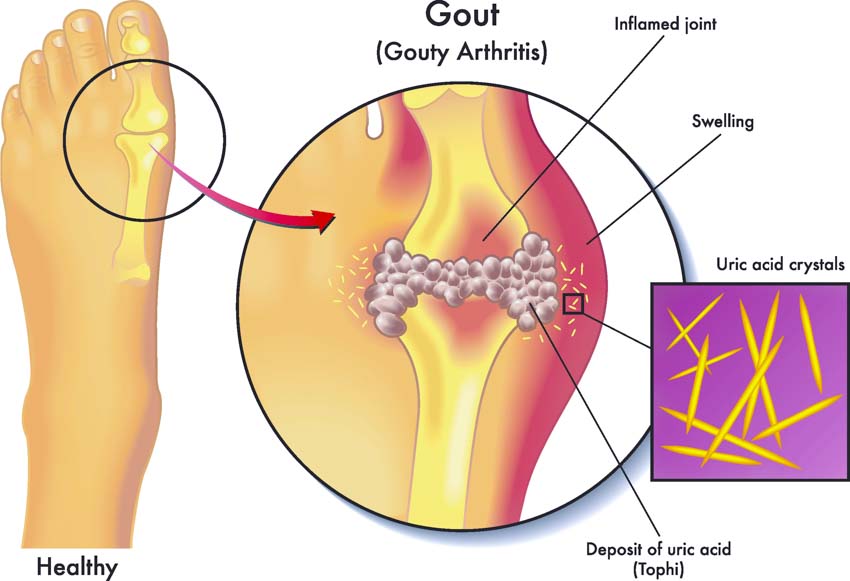
Acupuncture is more effective than a popular drug for the treatment of gout, a type of arthritis involving pain and inflammation due to a build-up of uric acid crystals in a joint. Dongguan Tangxia Guanhua Hospital researchers compared the efficaciousness of acupuncture with indomethacin (a non-steroidal anti-inflammatory drug) for the treatment of gout. Acupuncture produced a higher total effective rate than the medication, including greater reductions in pain, swelling, and redness. [1]
The study’s outcome measures included a VAS (visual analog scale) for pain, serum levels of uric acid and proinflammatory chemokine IL-8 (interleukin 8), and average temperatures of the affected joints. Both the acupuncture and drug groups experienced improvements following treatment and both showed improvements in clinical symptoms such as joint mobility, function, redness, and swelling.
Improvements in clinical symptoms were significantly greater in the acupuncture group (p<0.05) and the total effective rate in the acupuncture group was 86.96%, compared with 69.57% in the drug group. Acupuncture also caused fewer adverse reactions, with an incidence of just 2.17% compared with 23.91% in the drug group.
A total of 92 patients with acute gouty arthritis were assigned to either the drug group or acupuncture group using a randomized digital table. The drug group was comprised of 41 male and 5 female patients, ages 23–60 years (mean age 49.7 years). The acupuncture group was comprised of 42 male and 4 female patients, ages 19–60 years (mean age 48.6 years). There were no statistically significant differences in baseline characteristics between the two groups (p>0.05) at the outset of the human clinical trial.
Inclusion criteria consisted of a clinical diagnosis of gouty arthritis according to criteria set by the American College of Rheumatology 2001 Revised Guidelines, an acute flare-up of symptoms, and prospective patients having received no prior treatment for gouty arthritis. Patients were required to be ages 18–60 years and provide informed consent to participate in the study. Exclusion criteria were rheumatic or wind-dampness type arthritis, concurrent heart, liver, kidney, or lung disease, hematologic disorders, psychological disorders, and an allergy to the medication used in the study.
Patient Care
All patients were given standardized lifestyle and dietary advice to help them manage their condition. This included reducing their dietary intake of high-purine foods, organ meats, and alcohol. Patients were counselled on avoiding stress, cold temperature exposure, and overwork. All patients were advised to increase water consumption.
Patients in the drug group were prescribed indomethacin enteric-coated 75 mg tablets to be taken twice daily for 10 days. Patients in the acupuncture group did not receive the drug therapy but had acupuncture treatment administered at the following primary acupoints:
- Zusanli (ST36)
- Sanyinjiao (SP6)
- Yinlingquan (SP9)
- Quchi (LI11)
- Ashi points
Points were needled bilaterally, with the exception of ashi points which were needled on the affected side only. In addition to the primary points, secondary points were utilized according to each patient’s affected joint.
- For the 21 patients with knee pain, Yanglingquan (GB34), Xuehai (SP10), and Xiyan (MNLE16) were added.
- For the five patients with elbow pain, Hegu (LI4) was added.
- For the 19 patients with ankle pain, Kunlun (BL60) and Jiexi (ST41) were added.
- For the one patient with wrist pain, Yangchi (TB4), Waiguan (TB5), and Hegu (LI4) were added.
Patients were treated in a supine position using single-use, disposable acupuncture needles. The filiform needles were inserted following routine disinfection and, after obtaining deqi, were manipulated with a reinforcing-reducing technique incorporating lifting, thrusting, twisting, and rotating techniques. Needles were retained for 30 minutes and treatment was administered daily. Each course of care was comprised of five treatments, and a total of two courses were administered, separated by a two-day break.
Outcomes, Safety, and Discussion
Outcome measures for the study included a VAS for pain, serum uric acid and IL-8 levels, and temperatures of the inflamed joints (measured by infrared thermal imaging). Clinical symptoms such as joint mobility, redness, swelling, and joint function were also measured on a scale of 0–4, with higher scores indicative of more severe symptoms.
Mean pre-treatment VAS scores were 4.26 in the drug group and 4.31 in the acupuncture group. Following treatment, the scores fell to 1.61 and 0.78 respectively, indicating significantly greater reductions of pain in the acupuncture group (p<0.05). Mean pre-treatment uric acid levels were 519.92 µmol/L in the drug group and 525.06 µmol/L in the acupuncture group. Following treatment, uric acid levels fell to 437.28 µmol/L and 426.53 µmol/L respectively.
Mean pre-treatment IL-8 levels were 38.24 µg/L in the drug group and 38.81 µg/L in the acupuncture group. Following treatment, IL-8 levels fell to 26.23 µg/L and 26.04 µg/L respectively. Mean pre-treatment temperatures of the affected joints were 34.72°C in the drug group and 34.89°C in the acupuncture group. Following treatment, temperatures fell to 31.37°C and 31.20°C respectively. Both groups had significant improvements across all of these areas (p<0.05).
In terms of clinical symptoms, mean pre-treatment scores in the drug group were 1.57 for mobility, 1.92 for redness and swelling, and 1.63 for joint function. Corresponding scores in the acupuncture group were 1.59, 1.99, and 1.65. Following treatment, these scores fell to 0.89, 1.25, and 0.92 in the drug group and 0.56, 0.72, and 0.72 in the acupuncture group. Although both groups demonstrated improvements in clinical symptoms, they were significantly greater in the acupuncture group (p<0.05).
The total effective rates were calculated for each group. Patients whose clinical symptoms and uric acid levels had returned to normal were classified as recovered. Patients that showed improved symptoms and better uric acid levels were classified as improved. Patients that did not show any improvements in either area were classified as ineffective. In the drug group, there were 9 recovered and 23 improved patients, giving a total effective rate of 32 (69.57%). In the acupuncture group, there were 12 recovered and 28 improved patients, giving a total effective rate of 40 (86.96%).
Adverse reactions were monitored in both groups throughout the study period. In the drug group, there were 11 adverse reactions including nausea, vomiting, somnolence, and headaches. In the acupuncture group, there was one case of redness and swelling at the needle site which was mild and relieved by application of a hot compress. The incidence of adverse events in the drug group was 23.91% compared with 2.17% in the acupuncture group.
The results of this study indicate that acupuncture offers an effective and well-tolerated alternative to NSAIDs (non-steroidal anti-inflammatory drugs) for the treatment of gout. Acupuncture demonstrated the ability to reduce clinical symptoms and improve both serum uric acid and IL-8 levels. Also, acupuncture has a low risk of causing adverse reactions compared with indomethacin.
1. Chen Zhenfeng (2019) “Clinical Observation on Acupuncture Treatment of Acute Gout Arthritis” Chinese Medicine Research Vol.16(3) pp.75-78.


