
Acupuncture alleviates myospasms and pain due to spinal cord injuries. Second Affiliated Hospital of Heilongjiang University of Traditional Chinese Medicine researchers examined the effects of both acupuncture and electroacupuncture. In their clinical trial, both modalities produced significant patient outcomes. However, electroacupuncture edged out manual acupuncture with an 86.67% total effective rate. [1] Manual acupuncture scored a 79% total effective rate.
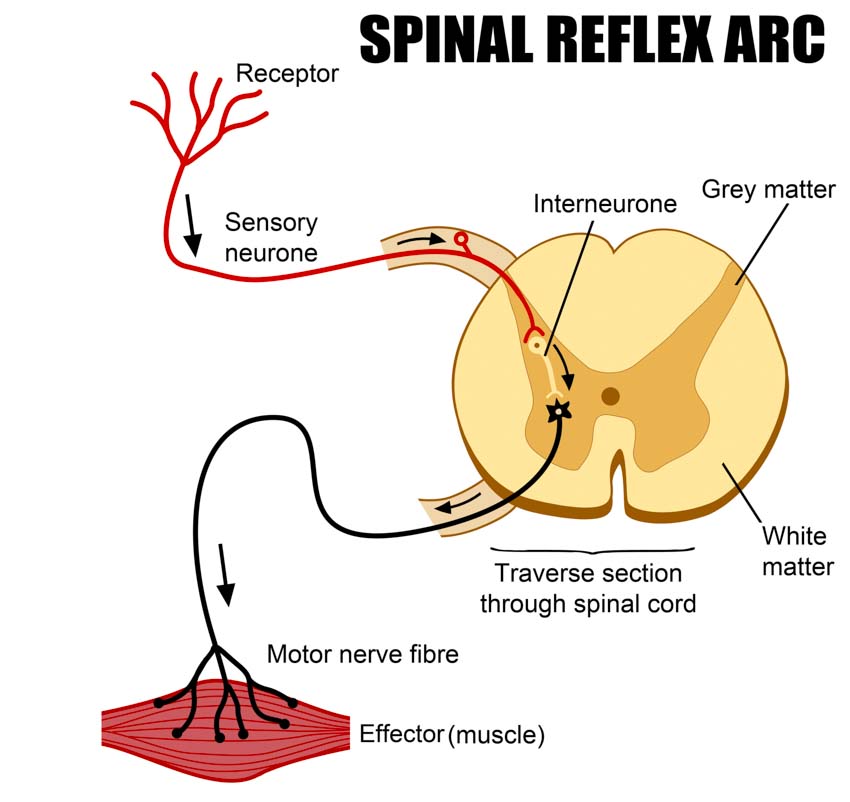
The researchers commented on the results. They note that acupuncture activates central nervous system GABA receptors and enhances motor neuron activity involved in nerve reflexes. The researchers comment that these improvements lead to reduced muscle tension and relief from myospasms.
Spinal Cord Injury (SCI) treatment often involves highly specialized scalp acupuncture protocols in the field of Chinese medicine. This is required due to the intractable nature of spinal cord injuries. Notably, Prof. Ming Qing Zhu is a prominent figure in the field of scalp acupuncture neurology. Prof. Zhu developed specialized scalp acupuncture zones and techniques that produce significant outcomes for patients suffering from paralysis and spinal cord injury related disorders.
The Heilongjiang University researchers varied from the scalp acupuncture approach and focused on standard body acupuncture channel points. At HealthCMi acupuncture continuing education, we recommend incorporation of the Prof. Zhu scalp acupuncture system into future investigations to improve patient outcomes. Also notable is the source of data for the outcomes. Heilongjiang University of Traditional Chinese Medicine is consistently a leader in research and publications in the field of acupuncture, including the text Syndromes of Traditional Chinese Medicine, Analysis of 338 Syndromes. The text is special because it includes all traditional Chinese medicine (TCM) differential diagnostic patterns. Chief compiler and president of Heilongjiang University, Prof. Huang Bing-Shan, personally presented the text in the USA at Five Branches University in Santa Cruz, California, in the early 1990’s.
Second Affiliated Hospital of Heilongjiang University of Traditional Chinese Medicine researchers used a sample size of 60 patients admitted into the hospital from January 2018 to December 2020. Patients were randomly divided into a manual acupuncture group and an electroacupuncture group, with 30 cases in each group.
Symptoms presented by patients included severe pain in the affected area, sudden onset of muscle spasms, increased muscle tension, hyperactive tendon reflexes, paroxysmal muscle spasms, joint contracture, and deformity. Based on a 6-level SCI measuring scale designed by the American Spinal Injury Association (ASIA), all patients were categorized into Level B (minimal movement) to Level D (active movement against resistance). Age range among patients was 25 to 75 years.
No patients had received any medicine that might cause muscular relaxation one month prior to the treatment. Blood tests, liver and kidney functions, electrocardiograms, and X-rays showed no irregularities that would interfere with the investigation, as a precondition of inclusion. Exclusion criteria were surgical history in the affected area, fever caused by infection, bone fractures, and severe peripheral nerve injuries.
Both groups underwent two weeks of treatment. Treatment was administered for 30 minutes, daily, for 6 consecutive days, followed by a one-day break. For the manual acupuncture group, 0.30 mm × 40 mm needles were applied perpendicularly using a mild reinforcing-attenuating method to achieve a deqi sensation. The following points were used in the procedure:
- LI15 (Jianyu)
- TB14 (Jianliao)
- TB10 (Tianjing)
- LI10 (Shousanli)
- TB5 (Waiguan)
- LI4 (Hegu)
- EX-UE9 (Baxie)
- ST31 (Biguan)
- SP10 (Xuehai)
- GB34 (Yanglingquan)
- GB39 (Xuanzhong)
- LV3 (Taichong)
In addition to the above treatment, the electroacupuncture group also received treatment on Jiaji (EX-B2) acupoints in the myopspasm area. Two pairs of Jiaji points were chosen at the upper and lower part of the affected area. Patients took a lateral or prone position. The needles were inserted using the same needling techniques as in the above group. After obtaining deqi, ipsilateral Jiaji points were connected to an electroacupuncture device, with the upper point linked to the positive electrode and the lower point to the negative. A sparse wave of 100 Hz was used. Pulse length was set to 0.5 ±0.15 ms.
To obtain this type of control with electroacupuncture, a specialized device is needed to control the pulse width. For example, the ITO ES-160 allows for this setting along with programmable treatment settings. At HealthCMi acupuncture CEUs, we mention this device, in particular, because it uses a symmetrical biphasic rectangular pulse and has the unique sweep mode plus standard settings such as burst, constant, surge, intermittent, etc. Notably, the smaller handheld model (ES-130) is very popular among acupuncturists. It lacks pulse width settings but shares the reliability of the ES-160.
Results were determined by several factors. The efficacy rate was calculated based on the Clinic Spasticity Index (CSI), Motor Assessment Scale (MAS), and the Barthel Index for Activities of Daily Living (ADL). Three levels were used to assess the efficacy rate:
- Significantly effective: CSI and MAS lowered by over 2 levels, Barthel upgraded by over 2 levels.
- Effective: CSI and MAS lowered by 1 level, Barthel upgraded by 1 level.
- Ineffective: CSI, MAS and Barthel indexes presented no change.
In the manual acupuncture group, 1 case was significantly effective, 20 were effective, and 9 were ineffective, contributing to a total efficacy rate of 70.00%. In the electroacupuncture group, 10 cases were significantly effective, 16 were effective, and 4 were ineffective, contributing to a total efficacy rate of 86.67%.
Globally, spinal cord injuries result in many cases of disability. Complications and impacts on daily living are often severe. Like all physicians, licensed acupuncturists look forward to medical breakthroughs that restore sensory and motor function to SCI patients. To date, no treatment program is 100% satisfactory. Surgery, drugs, and physical rehabilitation & training programs contribute to the armament of treatment modalities. Based on this research and many other investigations, acupuncture is an essential component for SCI patient recovery programs because acupuncture increases positive patient outcome rates.
Reference:
1. Clinical Observation on Treating Myospasm Induced by Spinal Cord Injury in 30 Cases, Tang Yizhou, Zhang Chong, Jiao Chuaxu,.etc, Jiangsu Traditional Chinese, Medicine, Volume 51, 2021.


