Acupuncture is an effective treatment modality for patients with carpal tunnel syndrome. Independent investigations confirm that acupuncture is more effective than usual care, including anti-inflammatory medications. Acupuncture successfully alleviates pain, inflammation, numbness, and restores motor dexterity. Electromyography confirms the results, including improvements across multiple parameters (e.g., median nerve sensory latency, sensory nerve conduction velocity, sensory amplitude, motor latency, motor nerve conduction velocity, motor amplitude).
About Carpal Tunnel
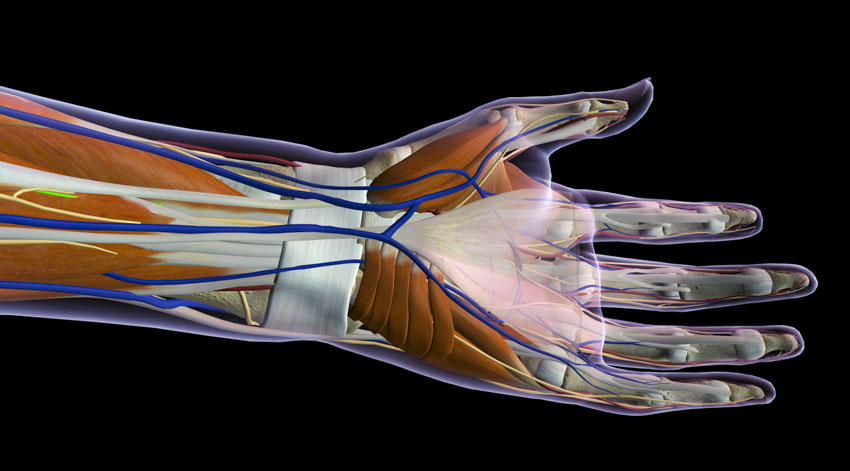
The carpal tunnel is a canal connecting the forearm and hand. Carpal tunnel syndrome pain and numbness is due to compression of the median nerve traveling through the canal. Researchers demonstrate that acupuncture benefits the median nerve and alleviates pain. Usual care for late-stage carpal tunnel syndrome (CTS) often includes surgery. Usual care treatment for early to mid-stage CTS typically involves pharmaceutical medications, physical therapy; or alternatively, acupuncture and tui na massage. [1–3]
Early diagnosis and intervention is crucial in mitigating median nerve damage and restoring nerve function. [4–5] Carpal tunnel braces may be used to relieve CTS symptoms, but may encumber patients by limiting hand movements. Acupuncture therapy preserves freedom of movement because braces are unnecessary. Acupuncture alleviates median nerve compression, in part, by reducing edema and accelerating axonal regeneration. [6] The axon is the lengthy threadlike part of a nerve cell carrying impulses. Additional research confirms that paraffin wraps combined with Traditional Chinese Medicine (TCM) herbs also promotes clinical improvements. [7]
Research teams provide a general overview of acupuncture for the treatment of CTS in their discussions. TCM differential diagnostic categories for carpal tunnel syndrome include wind-invasion of the muscles, cold-dampness affecting the ligaments, or qi and blood stasis blocking the channels. Local acupoint selections are commonly implemented to enhance the microcirculation of blood to the median nerve and carpal tunnel. The treatment principle is to restore the flow of qi and blood to the area, relieve pressure, promote regeneration, dredge the channels, and reduce tension. Common acupoints recommended for the treatment of CTS include the following:
- Daling (PC7)
- Neiguan (PC6)
- Yangxi (LI5)
- Hegu (LI4)
- Waiguan (TB5)
Affiliated Hospital of Liaoning TCM University
Researchers Wang Ye and Bai Yichen from the Affiliated Hospital of Liaoning Traditional Chinese Medicine University find acupuncture combined with herbal-paraffin treatment more effective than diclofenac, a nonsteroidal anti-inflammatory drug (NSAID). [8] In a 16-week clinical trial, two patient groups were compared. One group received acupuncture and herbal-paraffin treatment, the other received topical diclofenac. The results highlight that acupuncture with herbal-paraffin treatment produces greater pain relief and restoration of wrist function than a topical NSAID.
Treatment efficacy was evaluated on two levels: pain intensity and wrist function. The Numeric Pain Rating Scale (NRS), an 11-point numeric scale, was used to quantify pain intensity. In the NRS, the patient selects an integer from 0 to 10 (0 represents no pain and 10 represents maximum pain). Based on the NRS scores, pain reduction after treatment was calculated as a percentage using the following formula: [(pre-treatment NRS score)–(post-treatment NRS score)] / [pre-treatment NRS score] * 100%. Pain reduction efficacy for each patient was categorized into 1 of 2 tiers based on these percentages:
- Effective: NRS pain reduction percentage ≥50%.
- Ineffective: NRS pain reduction percentage <50%.
The pain reduction effective rate for each group was derived with the following formula: [Effective] / [Total number of patients in group] * 100%. Wrist function treatment efficacy was evaluated in accordance with “Guiding Principles for Clinical Study of New Chinese Medicines.” Based on clinical symptoms after treatment, the wrist function treatment efficacy for each patient was categorized into 1 of 4 tiers:
- Clinical recovery: Absence of hand numbness and wrist stiffness/weakness. Forearm able to function normally.
- Significantly effective: Hand numbness and wrist stiffness/weakness mostly alleviated. Forearm mostly able to function normally, albeit slight discomfort after intense movement/exertion.
- Effective: Hand numbness and wrist stiffness/weakness alleviated, but slight pain/discomfort persists. Or relapse within 6 months after clinical recovery.
- Ineffective: No improvement, or worsening, of hand numbness and wrist stiffness/weakness. [9]
Results
The wrist function treatment effective rate for each group was derived with the following formula: [Clinical recovery + Significantly effective + Effective] / [Total number of patients in group] * 100%. The acupuncture with paraffin treatment group recorded a 90% pain reduction effective rate and an 85% wrist function treatment effective rate. On the other hand, the diclofenac group recorded a 65% pain reduction effective rate and a 50% wrist function treatment effective rate. The data shows a marked difference (P<0.05) in performance between acupuncture with herbal-paraffin and diclofenac, in both pain reduction and wrist function recovery outcomes.
Design
The study was set up as a double-arm cohort. A total of 40 patients participated in the study. They were diagnosed and treated for CTS at the Affiliated Hospital of Liaoning Traditional Chinese Medicine University. The diagnostic criteria were the following:
- Numbness in median nerve sensory innervation area, or entire forearm. Pain, loss of sensation or other abnormal sensations in forearm.
- Varying degrees of median nerve damage detected via electromyography.
- Increase in numbness, pain or swelling at night or in the early morning, possibly awakening patient from sleep.
- Increase in numbness and pain after repetitive wrist movement, can be alleviated by flicking wrist. Condition worsens in winter compared to summer.
- Lacking strength to clench the fist or hold items.
- Myatrophy of the thenar eminence.
- Positive Tinel's sign or positive Phalen's maneuver.
Diagnosis was confirmed if the patient fulfilled either criteria 1 or 2, together with any one criteria from 3 to 5. [10] Patients were randomly divided into the treatment group and the control group, with 20 patients each. The treatment group received TCM paraffin treatment and acupuncture. The control group was given diclofenac sodium gel. Both groups received treatment for 16 weeks.
For the treatment group, TCM paraffin treatment was first administered, followed by acupuncture. Paraffin treatment was carried out with paraffin blocks and TCM herbal packets. The paraffin blocks were made by cutting 2–4 cm thick paraffin wax (40°C to 50°C) into 10 cm x 15 cm blocks. TCM herbal packets were made by mixing herbs and packaging the mixture into individual packets with gauze. The mixture was comprised of the following herbs:
- Sangzhi (30g)
- Ruxiang (15g)
- Haitongpi (20g)
- Moyao (15g)
- Guizhi (30g)
- Honghua (30g)
- Mangxiao (10g)
- Niuxi (20g)
- Fangfeng (20g)
- Shenjincao (30g)
- Tougucao (30g)
- Weilingxian (30g)
- Yanhusuo (30g)
- Baizhi (30g)
The packets were soaked in water for 10–20 minutes, then brought to a boil and stored for use. Immediately before treatment, the packets were heated to 40–50°C. TCM packets and paraffin blocks were only applied at a tolerable temperature for the patient. Warm TCM packets were applied externally around the wrist. Paraffin blocks were placed over the packets and molded to conform to the shape of the patient’s forearm. The assembly was then secured in place with cotton padding and left for 20 minutes before removal. After treatment, patients were advised to avoid exposing the treated area to cold temperatures. [11] The following primary acupoints were applied on the afflicted side only:
- Daling (PC7)
- Neiguan (PC6)
Secondary acupoints were added based on discomfort locations. For pain or numbness in the thumb, the following acupoints were added:
- Jingqu (LU8)
- Shaoshang (LU11)
For pain or numbness in the index finger, the following acupoints were added:
- Yangxi (LI5)
- Hegu (LI4)
For pain or numbness in the middle finger, the following acupoint was added:
- Waiguan (TB5)
For redness, swelling, and pain at the back of the hand, the following acupoints were added:
- Zhongzhu (KD15)
- Yemen (TB2)
- Wailaogong
For myatrophy or pain of the thenar eminence, the following acupoint was added:
- Yuji (LU10)
Patients were treated in either the supine or sitting position. Size 0.25 mm x 25 mm Hwato brand disposable sterile acupuncture needles (Suzhou Medical Appliance Factory Co., Ltd.) were used. After disinfection, needles were swiftly inserted into each acupoint, following standard insertion depths and TCM manipulation techniques. The above TCM combined therapy was administered once per day. A total of 4 treatment cycles were administered, whereby 1 treatment cycle was comprised of 4 weeks of treatment. Each treatment cycle was followed by a 2-day break. The control group was given diclofenac sodium gel, applied topically on the wrist at painful areas. An appropriate amount of gel was gently rubbed into the skin until absorbed, 3–4 times per day. In addition to the above treatments, all patients were also advised to practice the following habits in order to facilitate recovery and improve overall wrist health:
- Use a mouse that fits one’s hand size, and a comfortable mousepad, so that the wrist is sufficiently relaxed.
- Ensure that keyboard and mouse placement is not too high nor too low; positioning should be parallel with the vertically resting elbow height.
- Avoid prolonged repetitive forearm movement.
- Moderately practice holding weights and wrist extension exercises to increase wrist muscle strength. [12]
Qufu Shuyuan Clinic
Research by Wang Yundong from the Qufu Shuyuan Clinic published in the Journal of Clinical Medical Literature finds acupuncture more effective than carpal tunnel braces. Acupuncture outperformed carpal tunnel braces for improvement of nerve conduction velocity and for the alleviation of CTS symptoms. The following electrophysiological parameters were used to evaluate treatment efficacy: distal motor latency (DML), distal sensory latency (DSL), and nerve conduction velocity (NCV). For the sensory nerve conduction study, 0.05 ms rectangular pulses were sent from the middle of the palm (7 cm from the active recording electrode) and the wrist (14 cm from the active recording electrode), and the sensory nerve response picked up by the active recording electrode was recorded. The reference electrode was placed at the distal interphalangeal joint. For the motor nerve conduction study, a 0.05 ms rectangular pulse was sent from the wrist (8 cm from the active recording electrode at the thenar eminence), and the motor nerve response picked up by the active recording electrode was recorded. The reference electrode was placed at the dorsal aspect of the first metacarpophalangeal joint.
In addition to the above parameters, general treatment efficacy was also assessed by recording the Global Symptom Score (GSS) of each patient. The following 5 aspects were scored: pain, numbness, stinging, weakness or slow response, and sleep disruption. [14] Each aspect received a score on a scale of 0–10, wherein 0 indicates the absence of symptoms and 10 indicates severity. The total efficacy score was then derived as the sum of all 5 aspect scores.
The DMLs and DSLs showed no meaningful differences between both groups after treatment (P>0.05), and neither did patients improve significantly within their own groups. For reference, the acupuncture group had a mean pre-treatment DML of 4.2 ± 0.71 ms, which remained approximately the same after treatment, at 4.1 ± 0.70 ms (P>0.05). Likewise, the braces group had a mean pre-treatment DML of 4.1 ± 0.43 ms, which remained similar after treatment, at 4.2 ± 0.42 ms (P>0.05). Despite the DML and DSL results, the two groups performed differently with regards to NCVs and GSSs.
Nerve Conduction Improvements
The mean nerve conduction velocity (NCV) for the acupuncture group increased to 37.6 ± 8.3 ms after treatment, from a pre-treatment value of 35.1 ± 5.3 ms. The mean NCV for the braces group was 33.6 ± 5.8 ms before treatment and 33.2 ± 5.9 ms after treatment. Of the two groups, only the acupuncture group achieved significant improvement in NCV (P<0.05). Furthermore, the post-treatment NCVs were much higher with acupuncture than with braces (P<0.05).
Symptomatic Improvements
The acupuncture group recorded a mean Global Symptom Score (GSS) of 24.1 ± 8.1 before treatment and 14.6 ± 5.4 after treatment, signaling a significant improvement in wrist sensations and function (P<0.05). By contrast, the braces group recorded a mean GSS of 23.7 ± 8.9 before treatment and 22.5 ± 8.9 after treatment, presenting no significant improvement in wrist sensations and function (P>0.05). From the NCV and GSS scores, the researchers conclude that acupuncture outperforms braces regarding the improvement of nerve conduction, alleviating wrist pain, and restoring wrist motor function.
Design
The study was set up as a double-arm investigation. A total of 64 patients from Qufu Shuyuan Clinic participated in the study. They were diagnosed with CTS between June 2013 and June 2014. The following selection criteria were applied:
- Numbness in median nerve innervation area (thumb, index finger, middle finger, ring finger).
- Stinging pain in hand or wrist upon repetitive movement.
- Discomfort is relieved by changing hand position and flicking wrist.
- Slight to moderate symptoms.
The following exclusion criteria were applied:
- Cervical or multiple neuropathy.
- Pregnancy.
- Rheumatoid arthritis, diabetes, cognitive impairment, thyroid dysfunction.
- External injuries.
Participants were randomly divided into two groups: treatment and control. Both groups were equivalent in all relevant demographics (P>0.05), setting the basis for a fair comparison of results. The treatment group had 32 patients, 9 males, 23 females, mean age 41.7 ± 9.3 years. The control group had 32 patients, 7 males, 25 females, mean age 41.1 ± 9.6 years. The treatment group received conventional acupuncture. The control group was given carpal tunnel night braces, vitamin B1 and B6, and placebo (sham) acupuncture. Both groups underwent treatment for 4 weeks. The following acupoints were administered for the treatment group:
- Daling (PC7)
- Neiguan (PC6)
Size 0.25 mm x 40 mm acupuncture needles were used. A total of eight, 60-minute acupuncture sessions were conducted over the course of 4 weeks. Based on the data, acupuncture significantly outperforms carpal tunnel braces.
Dalian University Research
Dalian University researchers (Wang et al.) find acupuncture effective for the restoration of nerve function and improvement of sensory nerve related subjective sensations. [15] Wang et al. conducted a 20-day clinical trial administering conventional acupuncture to patients with slight to moderate CTS. Their results show that acupuncture quantifiably improves nerve function and effectively alleviates carpal tunnel numbness, stiffness, or weakness.
Treatment efficacy was evaluated by measuring median nerve sensory latency, sensory nerve conduction velocity, sensory amplitude, motor latency, motor nerve conduction velocity, and motor amplitude. A Dantec Keypoint-4 electromyography (EMG) system was used for nerve electrodiagnosis and testing temperature was 27–30°C. The normal reference range for nerve conduction values were in accordance with “Efficacy observation of non-surgical treatment mainly involving electroacupuncture in treating slight to moderate CTS” by Zhang Cuifang. In addition to the above values, the overall treatment efficacy was also evaluated. Based on symptoms, the treatment efficacy for each patient was categorized into 1 of 4 tiers:
- Clinical recovery: Palm numbness and wrist stiffness/weakness completely cured.
- Significantly effective: Palm numbness and wrist stiffness/weakness mostly cured.
- Effective: Palm numbness and wrist stiffness/weakness moderately cured.
- Ineffective: No improvement, or worsening, of palm numbness and wrist stiffness/weakness. [16]
The treatment effective rate for each group was derived with the following formula: [Clinical recovery + Significantly effective + Effective] / [Total number of patients in group] * 100%. The median nerve sensory latency was 3.9 ± 0.6 ms before treatment, and dropped to 2.7 ± 0.4 ms after treatment. Sensory nerve conduction velocity was 42.7 ± 7.2 ms before treatment, and sped up to 55.2 ± 6.6 ms after treatment. Sensory amplitude was 7.8 ± 2.6 mV before treatment, and increased to 9.2 ± 1.7 mV after treatment. All 3 parameters showed a meaningful difference after acupuncture treatment (P<0.05).
The results showed a similar trend for median nerve motor innervation. The median nerve motor latency was 5.0 ± 0.6 ms before treatment, and fell to 3.7 ± 0.7 ms after treatment. Motor nerve conduction velocity was 51.4 ± 5.4 ms before treatment, and increased to 63.5 ± 9.3 ms after treatment. Motor amplitude was 7.2 ± 2.6 mV before treatment, and increased to 10.7 ± 2.2 mV after treatment. All 3 parameters showed a significant difference after acupuncture treatment (P<0.05).
The above results show that acupuncture has significant and quantifiable efficacy in restoring nerve function, yielding both sensory and motor related clinical improvements. Also taking into account the high overall treatment effective rate of 86.67%, the data demonstrates that acupuncture benefits CTS patients by repairing nerve damage, thereby improving wrist function and relieving numbness.
The study was set up as a single-arm clinical trial. A total of 30 patients with slight to moderate CTS participated in the study. The participating patient pool consisted of 12 males, 18 females, between 47.5 ± 5.3 years, with durations of illness between 3 months to 2 years. A total of 15 patients had CTS on both wrists and 15 had CTS on one wrist. Patients were all diagnosed according to nerve electrodiagnostics, clinical symptoms, and signs. The diagnostic criteria for slight to moderate CTS were:
- No myatrophy or weakening of the thenar eminence.
- Nerve conduction study (Site of stimulation: wrist; Site of recording: abductor pollicis brevis) showed that median nerve terminal distal motor latency (DML) was ≤4.5 ms. [17]
Patients received acupuncture for 20 days. The following primary acupoints were selected for application on the afflicted side only:
- Daling (PC7)
- Neiguan (PC6)
The following secondary acupoints were applied to the afflicted side:
- Jianshi (PC5)
- Hegu (LI4)
- Laogong (PC8)
Size 0.25 mm x 40 mm filiform acupuncture needles were used. Patients rested in a supine position during acupuncture. After standard disinfection, needles were swiftly inserted. For Daling, gentle acupoint stimulation was administered. The needle was inserted towards the carpal tunnel and manipulated with lifting, thrusting, and rotation until deqi was achieved. For Neiguan, Jianshi, Hegu and Laogong, medium to strong attenuating stimulation was administered until soreness, numbness, and fullness were felt. After achieving deqi, needles were retained for 40 minutes, during which they were rotated once every 5 minutes. One session was administered per day, for 20 days.
Summary
Objective and subjective data indicates that acupuncture is effective for the treatment of carpal tunnel syndrome. According to the research covered in this article, common protocols involve the application of acupoints Daling (PC7) and Neiguan (PC6). Patients interested in learning more about treatment are recommended to contact local licensed acupuncturists.
References
1 Ye AP, Zou R. Efficacy observation of electroacupuncture combined with acupoint injection in treating CTS J. Shanghai Journal of Acupuncture and Moxibustion, 2014, 33(10): 941-942.
2 Zhang CF. Efficacy observation of non-surgical treatment mainly involving electroacupuncture in treating slight to moderate CTS J. Hubei Journal of Traditional Chinese Medicine, 2014, 36(10): 57-58.
3 Xia Q, Liu XW, Wang XL. Efficacy observation of using mainly electroacupuncture in treating CTS J. Chinese Acupuncture and Moxibustion, 2013, 33(8): 700-702.
4 Shi PQ, Yang HM. Efficacy observation of using Bo needling to treat CTS 108 cases J. Clinical Journal of Chinese Medicine, 2014, 6(27): 108-109.
5 Ren CH, Lei Q. Electrodiagnosis of CTS J. China Journal of Modern Medicine, 2004, 14(5): 102-103.
6 Tong S, Wang S, Sun ZR. Effect of acupuncture in mice in motor end-plate after sciatic nerve damage J. China Journal of Rehabilitation Medicine, 2007, 22(6): 533-534.
7 Wang Y, Li FS. Efficacy observation of TCM herbs paraffin treatment combined with ultrashort wave therapy in treating knee synovitis J. Chinese Archives of Traditional Chinese Medicine, 2015, 7(8): 1876-1879.
8 Wang Y, Bai YC. Treating Carpal Tunnel Syndrome by Acupuncture Combined with Chinese Medicine Paraffin J. Journal of Changchun University of Chinese Medicine, 2016, 32(3): 552-554.
9 Zou L, Mo JY. Observation care and prevention in treating slight to moderate CTS with TCM herbs fumigation and external application combined with ultrashort wave therapy J. China Medicine and Pharmacy, 2014, 6(12): 96.
10 Hu DQ. Clinical efficacy observation of needle-knife acupuncture in treating CTS D. Hangzhou: Zhejiang University of Traditional Chinese Medicine, 2014.
11 Zhang QY. Effect of laser acupuncture on CTS D. Guangzhou: Guangzhou University of Traditional Chinese Medicine, 2011.
12 Jin LQ, Lang BX. Efficacy observation of electroacupuncture combined with acupoint injection in treating early CTS J. Shanghai Journal of Acupuncture and Moxibustion, 2011, 7(7): 464-466.
13 Wang YD. Research on efficacy of TCM acupuncture for CTS J. Journal of Clinical Medical Literature, 2015, 2(5): 890-891.
14 Li Y, Zhu XY, Huang HY. Progress of CTS diagnosis J. Chinese Journal of Rehabilitation Theory and Practice, 2013, (3): 246-249.
15 Wang W, Tang W, Chi HT, Zhang J. Acupuncture in treating CTS 30 cases J. Journal of Clinical Acupuncture and Moxibustion, 2016, 32(5): 28-29.
16 Health Department of the General Logistics Department of the Chinese People's Liberation Army. Diagnostic standards and standards for clinical efficacy for clinical diseases S. Beijing: Military Science Publishing House, 1998: 390.
17 Gu YH, Zhang KL, Zhu Y, et al. Discussion on quantitative indicators of electrophysiology stages in CTS J. Chinese Journal of Hand Surgery, 2004, 20(3): 145-147.


